


Does Non-Surgical Spinal Decompression Actually Work? Surgery was recommended after four years of chronic disc injury.He chose conservative care first. His follow-up MRI changed the conversation entirely.
For many people living with chronic disc injuries, the path feels predictable. Pain begins in the lower back. Then the leg pain arrives. Sleep fractures. Sitting becomes something to endure. Training stops. And slowly, confidently, a surgeon’s referral arrives with a recommendation that feels both inevitable and terrifying: “you may need surgery.”
That was the reality facing one of our patients when he first walked through the doors of Optimal 365 in December 2025 — four years into a disc injury that had progressively narrowed his world.
A Four-Year History of Chronic Disc Injury
His imaging told a significant structural story: a large L3 disc extrusion alongside L4/L5 disc bulges — a multilevel pattern that placed consistent pressure on the surrounding nerve roots. But what the MRI could not fully capture was the cumulative functional toll.
- Large L3 disc extrusion with nerve root irritation
- L4/L5 disc bulges causing lower lumbar compression
- Severe, persistent lower back pain
- Right-sided leg pain and sciatica
- Difficulty sitting for any sustained period
- Seven months of complete cessation of gym training
- Sharp pain with bending, lifting, and twisting
- Heightened caution and avoidance with daily movement
Over time, the pain had become something larger than physical sensation. It had reorganised how he moved, how he planned his day, how confidently he inhabited his own body. Long drives became difficult. Simple activities carried a constant background awareness of threat.
After reviewing his imaging, his surgeon had recommended operative intervention. Before proceeding, he wanted to know one thing: did his body still have the biological capacity to recover without it?
Why Disc Injuries Become Chronic
The instinct when looking at a disc injury is to see it as a purely structural problem — material displaced, space reduced, nerve compressed. But chronic disc injuries are rarely that simple. They are biological and mechanical problems simultaneously.
When a disc becomes injured, a cascade of interconnected changes begins:
| 🔩 Mechanical compression Displaced disc material compresses surrounding ligament and adjacent nerve roots — reducing space and increasing irritation with every load. | 🔥 Inflammatory cascade Chemical release around the nerve root sensitises tissue well beyond the site of direct compression — widening the pain territory. |
| 🛡️ Protective guarding The body braces reflexively against anticipated pain, creating secondary stiffness that reduces movement and compounds the mechanical load. | 🔄 Impaired fluid exchange Reduced spinal movement limits the fluid cycling that keeps disc tissue nourished — accelerating degeneration in an already compromised segment. |
| ⚡ Nervous system sensitisation Pain thresholds lower over time. The nervous system amplifies signals that would previously have been sub-threshold. The volume increases without the stimulus needing to. | 📉 Progressive deconditioning Reduced activity diminishes the muscular support around the injured segment — removing the body’s own stabilising architecture from the equation. |
Over time, the body can become trapped in a self-reinforcing cycle: pain alters movement patterns, and altered movement patterns continue feeding the pain. Breaking that cycle requires addressing the mechanical, the biological, and the neurological simultaneously — not separately.
“The goal was not to mask pain. The goal was to improve the mechanical and physiological environment around the injured disc and the irritated nerve — and give the body the conditions it needed to do what it knows how to do.” |
The Treatment Protocol at Optimal 365
Following a thorough clinical assessment, a personalised eighteen-session programme was developed — two sessions per week over approximately nine weeks.
| Treatment Protocol at Optimal 365 |
|---|
| ✓ Non-Surgical Spinal Decompression Therapy |
| ✓ HPLT — High Power Laser Therapy |
| ✓ Progressive Rehabilitation Guidance |
| ✓ Two sessions per week |
| ✓ Eighteen sessions total over nine weeks |
WHAT IS NON-SURGICAL SPINAL DECOMPRESSION?
Non-surgical spinal decompression is a computer-controlled traction therapy designed to gently and precisely reduce compressive forces through the lumbar spine. Unlike older traction systems, modern decompression tables carefully regulate the force, angle, and cycling pattern of each session to minimise protective muscle guarding — the body’s reflexive resistance that has historically limited the effectiveness of manual traction.
The therapeutic aim is to create controlled, intermittent unloading of the spinal segment — reducing intradiscal pressure, improving fluid exchange and nutrient delivery into the disc, and reducing the mechanical irritation around compressed nerve roots. For some patients, this creates a window in which the nervous system and surrounding tissue can begin to settle, reorganise, and heal.
High Power Laser Therapy was added to address the inflammatory biology at the nerve root — using photobiomodulation to accelerate cellular repair and reduce the chemical sensitisation that had been amplifying his pain signals long after the initial injury.
The Follow-Up MRI
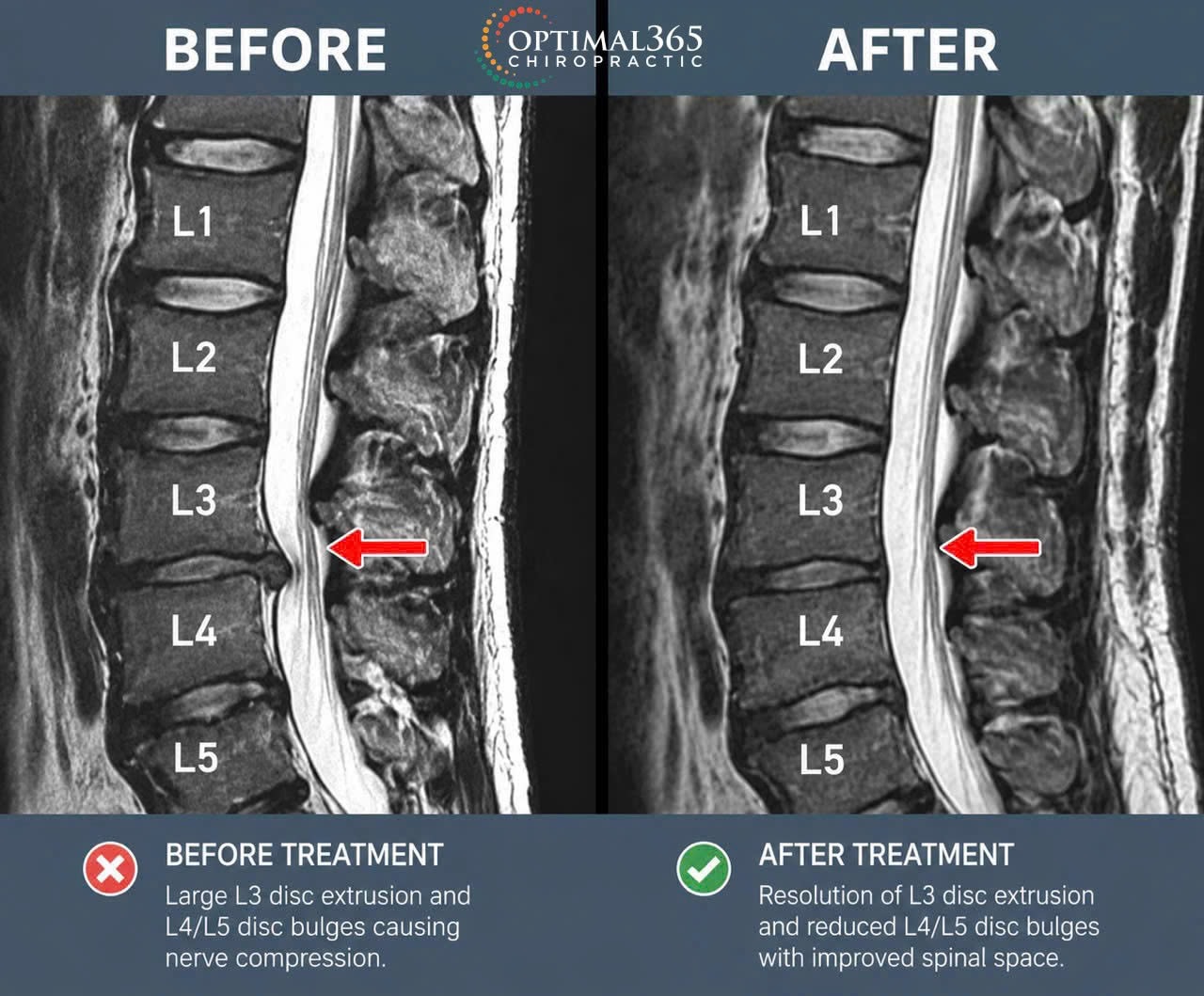
In April 2026, after completing his treatment programme, the patient underwent a repeat MRI of the lumbar spine. The radiological findings were significant.
| MRI FINDINGS — APRIL 2026 ✅ Resolution of the L3 disc extrusion. The large extruded fragment that had been compressing the adjacent nerve root was no longer present on imaging. ✅ Minimised L4/L5 disc bulging. Both levels showed meaningful reduction in size and displacement. After reviewing the updated imaging and clinical progress, his surgeon advised that surgical intervention was no longer required. |
Beyond the MRI — What Function Returned
Imaging confirms structural change. But imaging does not capture what it feels like to lift again, to drive without bracing, to sleep through the night, or to return to the gym after seven months away.
| Patient-Reported Outcomes at Discharge |
|---|
| ✓ Significant reduction in lower back pain intensity and frequency |
| ✓ Reduced right-sided leg pain and sciatica symptoms |
| ✓ Return to gym training — fully ceased for seven months prior |
| ✓ Improved tolerance to prolonged sitting |
| ✓ Restored confidence with bending, lifting, and daily movement |
| ✓ Greater overall quality of life and daily function |
This is the outcome that matters most. Not the T2-weighted signal change on a scan — but the capacity to move through life again with confidence and without constant anticipatory fear.
| “The body often has more capacity to recover than people realise — when the right environment is created around it.” |
Is Non-Surgical Spinal Decompression Right for Everyone?
The honest answer is no — and any clinician who tells you otherwise is not giving you complete information. Conservative care, however well-designed, does not override every clinical presentation.
Surgical intervention remains the appropriate pathway when there is:
| When Surgical Intervention Remains the Right Choice |
|---|
| → Progressive neurological weakness — foot drop, loss of grip, declining muscle function |
| → Loss of bowel or bladder control — a medical emergency requiring immediate attention |
| → Significant spinal cord compromise or structural instability |
| → Failure of appropriate, well-structured conservative care |
| → Structural severity incompatible with conservative resolution |
The clinical question is not surgery versus no surgery as a matter of principle. It is: does this patient, with this presentation, at this point in their history, have biological capacity remaining for conservative recovery — and has that pathway been appropriately explored?
For many patients, the answer is yes. And for those patients, a structured conservative programme — combining targeted decompression, neurological tissue support, and progressive rehabilitation — may provide a meaningful opportunity for recovery before any irreversible procedure is considered.
At Optimal 365, our role is to help determine, through thorough assessment and clinical reasoning, which patients are most likely to respond — and to design programmes that give the biology every advantage when they do.
If This Sounds Like Your Experience
If you are living with any of the following, it may be worth a clinical conversation before making permanent decisions:
- Chronic lower back pain lasting longer than 6–12 weeks
- Sciatica, leg pain, or pain that travels below the knee
- Diagnosed disc bulges, herniations, or extrusions
- Numbness, tingling, or altered sensation in the leg or foot
- Pain that significantly worsens with sitting, bending, or lifting
- Recurrent flare-ups that prevent training, work, or daily activity
- A surgical recommendation you would like to explore alternatives to first
The conversation does not have to begin with surgery. Sometimes the most important clinical question is simply whether the body still has room to heal — and what conditions it needs to do so.
Sometimes the right intervention is not about removing structure.
Sometimes it is about restoring the conditions that allow the body to find its own way back.




